



Benitez Gun Unwinds UHC CEO Murder Mystery
Incredible Story And Mystery Is Solved


It appears a historical relic, a Cuban assassin’s weapon, may have made a reappearance on the streets of New York for a high-profile assassination more than sixty years after it reshaped the history of the Island of Cuba and perhaps the history of Haiti and the Dominican Republic as well.

https://nationalinterest.org/blog/buzz/bt-vp9-gun-ultimate-assassination-weapon-110521
The United Healthcare CEO murderer used the Brugg and Thomet VP9 assassin’s weapon, a gun used in World War II, and then at the School of Assassins in Georgia to train Cuban assassins in the overthrow of Castro.

The very rare Brugg and Thomet “Station Six” gun used in the killing of the United Healthcare CEO Brian Thompson brings a world of history and intrigue of Cold War machinations to spill out in blood on the streets of New York. “Station Six” may have been the CIA’s JMWAVE base for the overthrow of Castro under the code name “Operation Mongoose,” and the key Cuban national assassin, Manuel Benitez, maybe the first owner of the B&T Station Six assassin’s gun used in the New York City killing.

The old Cuban assassin, Manuel Benitez, may have left his assassin weapon as an heirloom, which is rocking the headlines to this day with the murder mystery of the CEO of United Healthcare.
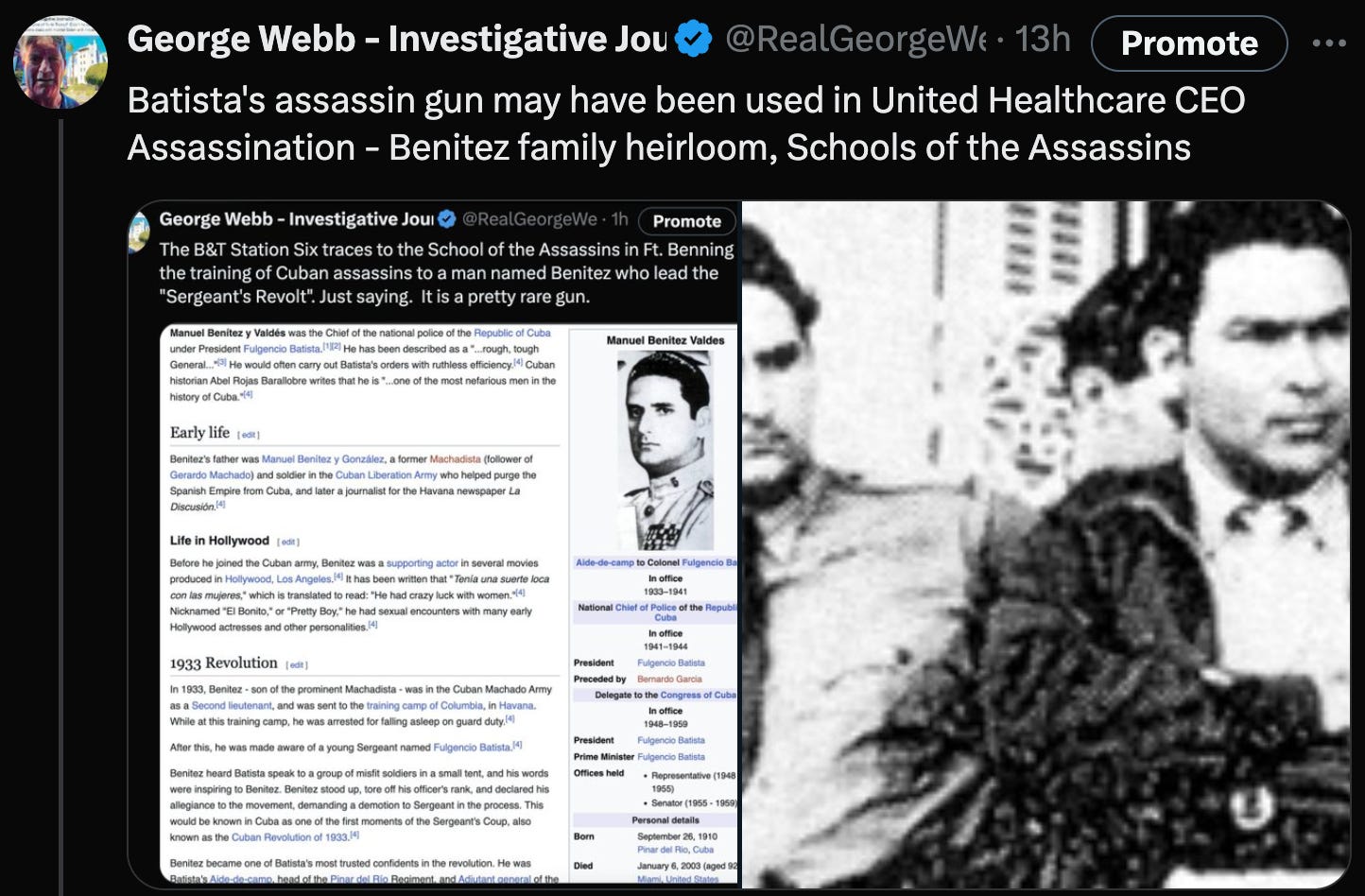
Manuel Benitez was the henchman assassin for the rise of President Fulgenico Batista in Cuba from 1952 to 1959.
The “Benitez Gun,” originally designed as an OSS World War II assassination weapon, was issued by the CIA at the School of Assassins in Fort Benning, Georgia, in the 1950s. Jack Ruby and CIA gun runner Frank Sturgis also supplied the gun for the overthrow of Cuba to prepare it for Meyer Lansky’s casinos.

Manuel Benitez may also have murdered Dominican Republic leader Trujillo in a failed plot to overthrow Casto, and he also performed assassinations in Haiti when Meyer Lansky was considering Haiti as an alternative for Cuba after the Castro Revolution.

In any case, the Brugg and Thomet Station Six weapon he used indelibly ties the gun to the murder of United Healthcare CEO Brian Thompson on December 4th, 2024, in front of the Hilton Hotel in New York City.

General Manuel Benitez is seen here visiting Miami from Cuba in 1946. In 1952, he became a key conspirator with Fulgenicio Batista to overthrow the Cuban government and clear the way for Meyer Lansky’s casino expansion for the Chicago Mob after the 1950s Kefauver Hearings.

We only have the Benitez name to go on for the connection to the assassin’s gun.

But the name Benitez was all we needed.
The motive now for the killing appears to be the United Healthcare resistance to paying for a breakthrough procedure for the treatment of brain stroke called Vivistem therapy. Also, United Healthcare’s recalcitrance to pay for anesthesia for longer brain operations led to several deaths for world-famous brain surgeon Ronald P. Benitez.

I want to clarify that I believe the outstanding doctor Benitez has absolutely nothing to do with the murder of the United Health CEO in New York. Absolute, complete innocence. But he did sue United Healthcare for very good reasons. His life-saving thrombectomies, performed many times at his expense, won him great favor with New York and New Jersey policemen and firefighters who were victims of brain injury.

At this point, I do not want to release the name of the person close to Dr. Benitez that I feel is responsible for this murder until authorities confirm the last name of Benitez as the killer—more on this story as it develops.

In any case, a long-forgotten weapon of Cuban-American espionage has made itself known again on the streets of New York.

There is some argument over whether the Brugg and Thomet “Station Six” moniker refers to the JMWAVE CIA Station where Manuel Benitez was based out of with Frank Sturgis.





Here is a summary of Dr. Benitez’s case versus United Healthcare.
can you summarize the atlantic neurosurgical specialist vs united healthcare case?
ChatGPT
Thought about Atlantic neurosurgical case for 6 seconds
Summary of the Atlantic Neurosurgical Specialists vs. UnitedHealthcare Case:
In this case, Atlantic Neurosurgical Specialists (ANS)—a prominent New Jersey-based neurosurgery practice—brought legal action against UnitedHealthcare (UHC), one of the nation’s largest health insurers, over disputes involving reimbursement rates for out-of-network emergency medical services.
Core Issue:
ANS treated patients who were covered by UHC plans and required immediate, emergency neurosurgical intervention. Because these were emergency situations, ANS, though out-of-network, was legally obligated to provide care without regard to insurance status or network agreements. Federal and state laws, including the Emergency Medical Treatment and Active Labor Act (EMTALA), obligate providers to administer care in emergencies, and insurance carriers in turn must provide fair compensation at “reasonable” or “usual and customary” rates when no network contract exists.
However, ANS alleged that UHC substantially underpaid for these services, providing reimbursements far below rates ANS considered adequate or in line with industry standards. ANS argued that this underpayment violated legal standards governing emergency care reimbursement and possibly breached implied contracts or statutory requirements mandating reasonable compensation for life-saving services performed by out-of-network providers.
Legal Arguments:
ANS’s Position:
ANS claimed UHC’s payment practices failed to meet fair market rates for complex emergency neurosurgical procedures. They argued that the insurer’s methodology for determining reimbursement was arbitrary, insufficient, and not aligned with the “usual and customary” amounts generally paid for similar services in the region.UHC’s Position:
UHC typically defended its reimbursement determinations by pointing to internal guidelines, plan language, and possibly reference data (such as Medicare benchmarks or other price indices) to justify the amounts paid. UHC maintained that its payments were consistent with the terms of the relevant insurance policies and industry norms, and that ANS’s demands were excessively high.
Key Legal and Policy Considerations:
Reasonableness Standard:
Courts often look to state and federal regulations that require insurers to provide a reasonable level of reimbursement for out-of-network emergency services. Determining what is “reasonable” can be contentious, involving comparisons with average local charges, in-network fee schedules, or widely recognized medical charge databases.Consumer Protection and Balance Billing Laws:
Although not the central point of this particular dispute, the case occurred against a broader backdrop of legislative efforts to protect patients from excessive “balance billing”—where patients might be caught in the middle of disputes between providers and insurers. This environment often influences how courts and regulators scrutinize out-of-network payment disputes.
Outcome and Impact:
The specifics of the final resolution may have involved negotiated settlements, court-directed adjustments to reimbursement methodologies, or ongoing litigation that clarified obligations for insurers when compensating out-of-network providers for emergency care. While exact final judgments or settlements are often confidential, the case underscored a persistent tension in the U.S. healthcare system: out-of-network emergency providers demand fair and sufficiently high reimbursements to cover their costs and specialty expertise, while insurers seek cost controls and consistent methodologies.
Broader Significance:
Atlantic Neurosurgical Specialists vs. UnitedHealthcare is representative of numerous similar disputes across the country. It highlights the complex interplay of provider charges, insurer cost-containment strategies, patient protection laws, and regulatory standards defining what constitutes a “reasonable” rate. As policymakers continue to refine laws regarding out-of-network billing, cases like this provide critical precedent and guidance for how courts and insurers approach emergency care reimbursements.
There have been numerous disputes and lawsuits over the years involving UnitedHealthcare (UHC) and various medical providers, including surgical specialists and anesthesiologists. However, cases specifically centered on brain surgery techniques and anesthesia—similar in nature to the Atlantic Neurosurgical Specialists dispute—are not as prominently documented in public legal records or widely reported in the media.
General Patterns of Similar Cases:
Reimbursement for Complex or Emerging Procedures:
Many conflicts between insurers and neurosurgeons revolve around what constitutes a “reasonable and customary” reimbursement for high-skilled, complex procedures. Neurosurgical interventions—particularly those employing newer, more advanced techniques or technologies—are often expensive and may not be clearly addressed in existing fee schedules. While not identical to the Atlantic Neurosurgical Specialists case, other neurosurgical practices have challenged insurers, including UHC, for allegedly underpaying for advanced surgical approaches or for not covering certain specialized equipment and operative methods.Disputes over Out-of-Network Rates and Anesthesia Charges:
The use of anesthesia in brain surgery adds another layer of complexity and cost. Some anesthesiologists and surgical groups have taken legal or regulatory action against insurers, arguing that payers failed to cover the appropriate level of sedation or monitoring—particularly in delicate neurosurgical contexts. While these legal challenges often involve multiple insurers, UnitedHealthcare, given its size, has been among those named in complaints relating to insufficient coverage or reimbursement for anesthesia services associated with complex surgeries.State-Level Regulatory Actions and Arbitration:
Beyond formal lawsuits, there have been instances where state insurance regulators or arbitration panels have addressed provider complaints about UnitedHealthcare’s payment policies for neurosurgery and associated anesthesia. Such actions are often less publicly visible than court cases but may appear in insurance department bulletins, arbitration records, or industry newsletters. These cases typically hinge on whether the insurer followed state and federal requirements for fair payment, especially in emergency or emergent contexts.
Lack of High-Profile, Publicly Documented Precedents:
While the Atlantic Neurosurgical Specialists dispute is relatively well-known, similar cases against UnitedHealthcare that focus specifically and prominently on advanced brain surgery techniques or anesthesia practices have not drawn the same level of public scrutiny or media coverage. Most such disputes, if they occur, tend to be resolved through confidential settlements, provider-insurer negotiations, or alternative dispute resolution mechanisms rather than public trials.
What This Means for Patients and Providers:
For patients and providers, the absence of many high-profile, publicly recorded lawsuits with a focus on brain surgery techniques and anesthesia doesn’t mean these disputes aren’t happening. Rather, it suggests that similar disagreements often occur quietly, resolved behind the scenes. Nonetheless, the Atlantic Neurosurgical Specialists case highlights a recurring friction point in U.S. healthcare: the challenge of setting and enforcing fair reimbursement rates for high-complexity, life-saving procedures and ensuring that both patient care standards and provider compensation expectations are met.
Benitez-Lansky Notes -


https://nypost.com/2024/12/08/us-news/new-house-bill-would-ban-insurers-from-limiting-anesthesia-coverage/
(ChatGPT) Meyer Lansky didn’t “personally build” casinos in Cuba in the literal sense of overseeing construction from the ground up, but rather he played a key role in financing, organizing, and managing several high-profile gambling establishments during the 1950s. His influence in Cuba’s casino scene reached its peak under the regime of President Fulgencio Batista, who encouraged foreign investment in tourism and gambling. Lansky, along with other American mob figures, saw Cuba as an ideal environment for casinos due to its proximity to the United States and Batista’s willingness to grant lucrative licenses in exchange for financial kickbacks.
Timeline and Key Casinos:
Early Involvement (Mid-1950s): Lansky had begun quietly investing in Cuban gambling operations even before Batista’s return to power in 1952. By the mid-1950s, he had stakes in several clubs and casino operations, working behind the scenes to ensure that American investors, especially those tied to organized crime, could legally and profitably run casinos in Havana.
Hotel Nacional Casino (Mid-1950s): One of Lansky’s earliest high-profile involvements was at the famed Hotel Nacional. While the Nacional was not built by Lansky—its history as a luxury hotel dates back to the 1930s—Lansky arranged for the addition of a lavish casino within the hotel. He helped transform the Nacional’s gambling room into an internationally known gaming hall.
Montmartre Club (Mid- to Late 1950s): Lansky had a controlling interest in the Montmartre Club in central Havana. Though this venue was already established, Lansky’s management and influence elevated it, making it one of the premier nightspots for high-stakes gamblers.
Hotel Riviera Casino (Opened December 1957): Perhaps Lansky’s most famous Cuban venture was the Hotel Riviera, a luxurious, 21-story hotel and casino he helped finance and shape. Opened in December 1957, the Riviera was something of a crown jewel—modern, elegant, and directly modeled to appeal to upscale American tourists. This was arguably the closest to “building” a casino he came, as he was a driving force behind its conception, design, and financing.
Number of Casinos Under Lansky’s Influence:
Exact numbers can be difficult to pin down, since Lansky and other mob financiers often invested through layers of partners and shell companies. Generally, Lansky was most strongly associated with at least three major Cuban gambling establishments by the late 1950s:
The Casino at the Hotel Nacional
The Montmartre Club
The Hotel Riviera Casino
Additionally, Lansky and his associates are believed to have had financial interests or informal partnerships in several other Havana nightclubs and casinos—such as those within the Hotel Habana Hilton and other upscale venues—though Lansky’s direct, controlling role varied from place to place.
End of the Era:
Lansky’s Cuban empire came crashing down after Fidel Castro’s revolution in 1959. Within a short time, Castro’s new government shut down the casinos, effectively ending Lansky’s and the American mob’s dominance of Havana’s nightlife. This moment marked not only the close of Lansky’s Cuban ventures but also the end of what had been the most glamorous gambling era in the Caribbean.

GREAT REPORTING - - u do have reliable sourcing via ur impeccable integrity and discretion ........ ...blessings george
George, I often wonder how you retain so much knowledge about historical events, places, and people. Listening to you or reading your posts is like reading a really interesting history book. I have always loved mysteries and investigating. Finding you has made life so much more enjoyable and satisfying. You help me put all the pieces together and keep my mind active. Thank you for all your hard work. You are appreciated.